Quick Summary
- Irritable Bowel Syndrome (IBS) affects 5-10% of people globally and is driven by the Gut-Brain Axis, not just digestion.
- Diagnosis relies on Rome IV Criteria focusing on pain patterns linked to bowel movements.
- Treatment ranges from Low-FODMAP Diet (50-76% improvement) to Gut-Directed Hypnotherapy (70-80% success).
- New biomarker tools like VisceralSense™ can now predict treatment response with 85% accuracy.
- Serotonin levels play a massive role, with 95% produced in the gut influencing mood and motility.
For years, we were told irritable bowel syndrome was just "nerves" or that our stomachs were too sensitive. That explanation feels dismissive when your life is interrupted by cramps or urgent trips to the bathroom. In reality, there is a complex biological highway running right through your abdomen. This isn't metaphorical-it is anatomical. Your digestive system talks directly to your brain, and when that conversation goes wrong, IBS happens. Understanding this link changes everything because it means treating your gut requires addressing your nervous system, not just taking a pill for diarrhea.
The science has shifted dramatically. We now know the condition is defined by a breakdown in communication signals between your gut and your brain. When stress hits, your gut might spasm. When you eat certain foods, your nerves might overreact to gas bloating as pain. It is a two-way street where the traffic gets jammed. By recognizing these pathways, you can move away from guessing games and toward targeted strategies that actually calm the system down.
How the Gut-Brain Axis Works
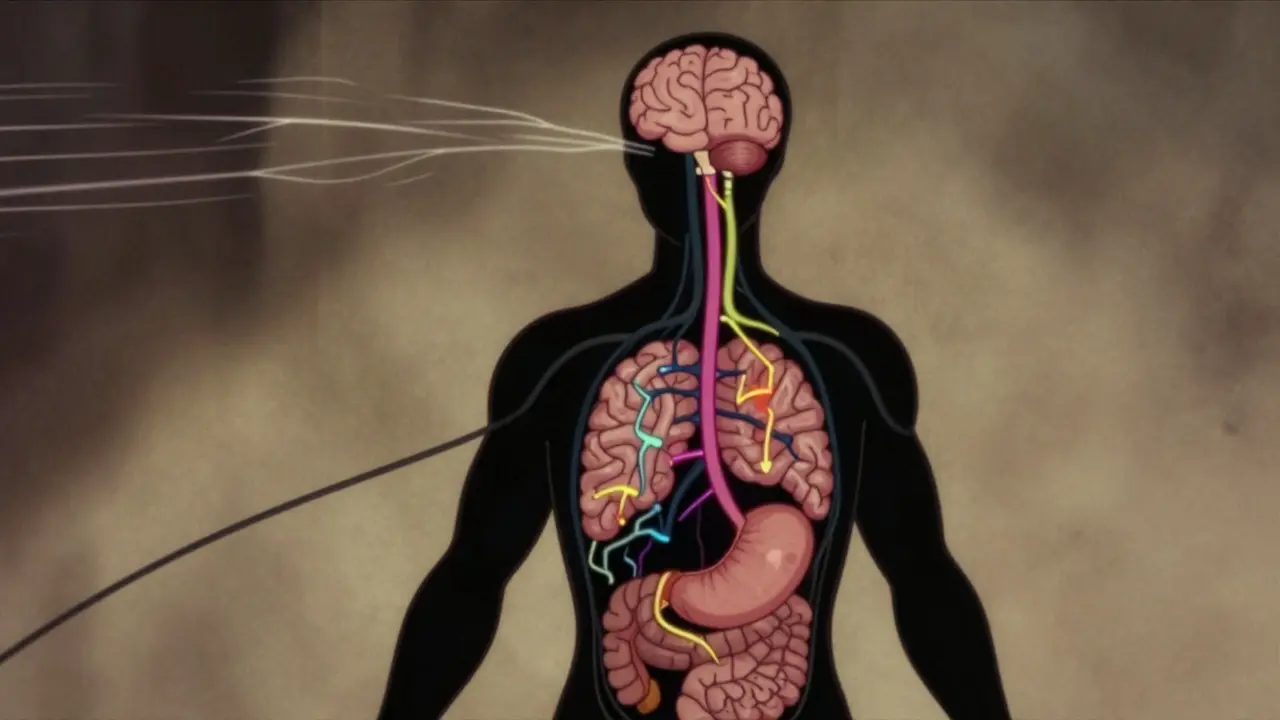
To fix the problem, you have to see the machinery. Think of the gut-brain axis as a control center connecting three main systems: your brain (Central Nervous System), your gut nerves (Enteric Nervous System), and the microbes living in your intestines. They communicate using chemical messengers called neurotransmitters. You probably know them for mood regulation, but their biggest factory is actually located in your stomach lining.
Consider the vagus nerve. This thick cable connects your brainstem to your abdominal organs. If your gut sends a distress signal, your brain interprets it immediately, often triggering anxiety. Conversely, high stress causes the brain to fire signals back to the gut, speeding up or slowing down movement. In people with IBS, the volume on these signals is turned way up. A normal amount of gas becomes painful; a small stress trigger triggers a full bowel movement. Researchers have found specific structural changes in the brains of IBS patients, such as altered thickness in the insula region which processes sensations from internal organs.
The Chemical Messengers Driving Symptoms
If the pathway is the wiring, serotonin is the electricity powering it. While we associate serotonin with happiness, 95% of your body stores it in the intestinal epithelial layer, not the brain. Here, it controls muscle contractions and fluid secretion. Studies show patients with diarrhea-predominant IBS (IBS-D) have significantly higher mucosal serotonin levels-averaging 45.7 ng/mg protein compared to 28.4 ng/mg protein in healthy individuals. Excess serotonin tells your bowel to move faster than intended, leading to urgency. For those with constipation (IBS-C), the issue is often reduced availability, leaving things moving too slowly.
Dopamine and GABA also play supporting roles here. Dopamine handles reward and motility speed, while GABA helps modulate pain sensitivity. When these chemicals get out of balance, the result is visceral hypersensitivity. Your nerves become like exposed wires; they should sense pressure, but instead, they scream when there is merely a mild touch. This explains why standard painkillers rarely work well-the pain is generated by nerve signaling errors rather than tissue damage like inflammation seen in Crohn's disease.
| Chemical Messenger | Primary Function | Effect in IBS-D | Effect in IBS-C |
|---|---|---|---|
| Serotonin | Motility & Fluid | Increased levels cause rapid transit | Decreased availability slows transit |
| GABA | Pain Modulation | Reduced inhibition leads to pain sensitivity | Reduced inhibition leads to pain sensitivity |
| β-Endorphin | Natural Painkiller | Lowered monocyte levels increase pain | Lowered levels correlate with discomfort |
Diagnostic Standards: The Rome IV Criteria
Before starting any treatment, you need a solid diagnosis to rule out other conditions like celiac disease or inflammatory bowel disease. Doctors rely on the Rome IV Criteria, established in 2016, to identify the syndrome accurately. It is strict by design to avoid misdiagnosis. The core definition centers on recurrent abdominal pain occurring at least one day per week for the last three months.
This pain must be associated with at least two of the following symptoms:
• Relation to defecation (pain improves or worsens after a bowel movement).
• Change in stool frequency (you are going much more or less often than usual).
• Change in stool form (appearing lumpy, hard, watery, or mushy).
Meeting these benchmarks confirms the diagnosis is functional disorder related to motility and sensation rather than organic damage to the tissues.
Dietary Modifications: Beyond the Basics
What you eat fuels this complex system. The most proven dietary intervention is the Low-FODMAP Diet. FODMAP stands for Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols. These are specific carbohydrates found in foods like onions, garlic, wheat, and apples that draw water into the gut and ferment rapidly. In a healthy gut, bacteria handle this easily. In an IBS gut, the fermentation creates gas bubbles that distend the intestine, triggering the sensitive nerves we discussed earlier.
Clinical trials show this diet leads to symptom improvement in 50% to 76% of patients. However, it requires discipline. It involves an elimination phase lasting 4 to 6 weeks where you cut all high-FODMAP foods completely, followed by a reintroduction phase. Many people find this difficult to maintain, but working with a dietitian is crucial. Skipping the reintroduction step can lead to nutritional deficiencies. You want to identify specifically which sugars trigger you, not stay restricted forever.
Targeting the Brain to Heal the Gut
If the gut cannot heal itself, calming the brain can help. Gut-Directed Hypnotherapy has emerged as one of the most effective non-drug treatments. It uses guided imagery to reset the way the brain perceives gut signals. Randomized controlled trials indicate a response rate of 70-80%, significantly higher than standard medical care alone (35-40%). This works because it desensitizes the central nervous system's reaction to normal gut movements.
You can imagine it as turning down the volume on the amplifier. Sessions typically take 7-12 visits, often with a cost between $1,200 and $2,500 out of pocket. While expensive, the effects often persist long-term. For those unable to access clinical hypnosis, biofeedback devices or even mindfulness meditation apps can offer partial benefits by lowering overall cortisol levels, which reduces the stress-induced spikes in gut signaling.
Medications Targeting the Axis
When lifestyle changes aren't enough, pharmaceutical options specifically designed for the gut-brain axis are available. These drugs don't just treat symptoms; they adjust the chemistry.
For IBS-D, Alosetron blocks serotonin receptors (5-HT3), reducing pain and diarrhea. It shows a 50-60% improvement in global symptoms for women but carries a risk of ischemic colitis, limiting its use.
For IBS-C, Prucalopride activates serotonin receptors (5-HT4) to boost gut movement, showing 45-55% improvement in constipation symptoms.
Recent developments include Etrasimod, a sphingosine-1-phosphate receptor modulator recently tested in Phase III trials. It showed a 52% improvement in composite scores versus 31% for placebo. This represents a new frontier in blocking the inflammatory pathways involved in the brain-gut dialogue. Always discuss side effects with a gastroenterologist, as medications affecting serotonin require careful monitoring.
The Microbiome Factor and Emerging Tools
Your gut hosts trillions of bacteria that produce their own chemicals. Dysbiosis, or an imbalance in these microbes, contributes to inflammation. While probiotics vary wildly in effectiveness, specific strains like Bifidobacterium infantis 35624 have shown 30-40% improvement in global symptoms. Fecal microbiota transplantation (FMT) is another option, though results depend heavily on the donor quality.
New diagnostics are changing the landscape. In 2023, the VisceralSense™ panel launched, measuring 12 microbial metabolites and neurotransmitter ratios. It predicts treatment response with 85% accuracy based on a 1,200-patient cohort. Moving forward, personalized medicine will likely rely on these biomarkers. Instead of trying random diets, patients may soon receive a report telling them exactly which pathway is broken and which supplement or drug will fix it.
Can stress physically cause my stomach pain?
Yes. The gut-brain axis communicates bi-directionally via the vagus nerve. Stress hormones like cortisol alter gut motility and heighten pain sensitivity in the enteric nervous system, making normal digestion feel painful.
Is the Low-FODMAP diet permanent?
No. It is designed as a temporary elimination phase (4-6 weeks) followed by systematic reintroduction. Long-term restriction reduces bacterial diversity and nutrient intake.
Why does seratonin matter for digestion?
95% of the body's serotonin is produced by enterochromaffin cells in the gut. It regulates the strength of gut wall contractions and controls how much fluid is released during bowel movements.
How effective is gut-directed hypnotherapy?
Studies show a 70-80% response rate, outperforming standard medication which sees around 35-40% improvement. Effects are often sustained six months after stopping sessions.
Are there biomarkers to test for IBS subtypes?
New tools like VisceralSense™ measure microbial metabolites to predict IBS subtypes (D vs C) and treatment response with up to 85% accuracy in pilot cohorts.
Comments (9)
-
Richard Kubíček March 27, 2026
It really changes the perspective when you realize your stomach has its own nervous system entirely. Most people just think digestion is mechanical until they experience the visceral pain directly. I always found the idea of serotonin being gut-based fascinating before reading this breakdown. It makes sense why stress manifests physically so often during hard weeks at work. We need more education on how mental states affect our biology directly like this. Understanding the vagus nerve function helps explain why relaxation techniques actually help bowel movements too. It is not just about what goes into the mouth but how the system processes signals downstream. Treatment options looking this comprehensive gives hope for those stuck in diagnostic limbo. Hopefully doctors start prescribing hypnotherapy more frequently given these success rates. The biological evidence is overwhelming now that research has moved past dismissive theories.

-
gina macabuhay March 29, 2026
People seem to love blaming their own physiology on abstract concepts rather than acknowledging poor lifestyle choices frankly. If one ate properly most of these issues would not manifest with such severity in the first place. It is insulting to suggest that medication fixes what self-discipline should resolve initially. The article glosses over how many patients are simply misdiagnosed because they refuse basic dietary accountability. Blaming the brain axis is convenient when one does not want to change actual habits. This narrative enables dependency on pharmaceuticals rather than personal responsibility. We need less sympathy for laziness disguised as medical complexity honestly.

-
Monique Louise Hill March 29, 2026
Your attitude is genuinely toxic and unhelpful to anyone actually suffering through this nightmare daily! 😠

-
Monique Ball March 30, 2026
This detailed breakdown of the Low-FODMAP protocol is absolutely critical for anyone navigating the confusing maze of chronic digestive issues!!! It is so important to recognize that the elimination phase cannot be skipped without risking severe long-term health complications down the line!!! Many well-meaning individuals fall into the trap of permanent restriction which ultimately destroys their gut microbiome diversity completely!!! The success rate figures mentioned in the text are truly remarkable and provide a beacon of hope for sufferers worldwide!!! 😊 Working alongside a certified professional is non-negotiable when implementing such a strict dietary regimen successfully!!! Without that expert guidance people often miss the subtle signs indicating a specific sugar trigger is finally identified correctly!!! Gas accumulation described here explains why simple bread intake can feel like an explosion inside the abdominal cavity violently!!! 😩 We need to normalize these conversations so patients feel validated by their doctors instead of dismissed by outdated thinking!!! 🌟 Scientific validation gives us the tools needed to reclaim control over our physical well-being once and for all!!! 💡 Every statistic cited supports the urgent need for broader adoption of these evidence-based therapeutic strategies immediately!!! 💉 Pharmaceutical costs should never replace the foundational healing power of a balanced microbial environment within the intestine!!! 📢 Sharing this knowledge reduces the isolation felt by so many struggling silently with invisible symptoms daily!!! 🧠 The psychological impact of feeling powerless is heavy but education lifts that burden incredibly high!!! 📖 Reading this made me realize how many years were wasted guessing which foods were making things worse unnecessarily!!! ✨ Please prioritize learning the reintroduction phase because that is where real dietary freedom is actually found permanently!!! 🚀 This post deserves maximum visibility so that others find their path to relief sooner rather than later!!!

-
Austin Oguche March 31, 2026
The emergence of VisceralSense represents a significant shift toward personalized medicine protocols globally. Many regions rely heavily on trial error methods which waste valuable time and resources unnecessarily. Having an accuracy rate of eighty five percent allows for targeted interventions that respect individual patient biology fully. This tool could standardize care across different healthcare systems effectively. Precision diagnostics should become the norm rather than the exception moving forward soon. It bridges the gap between subjective symptom reporting and objective physiological measurement nicely.

-
Sarah Klingenberg April 2, 2026
I really hope more clinics adopt these testing panels for everyone who suffers :( The old way of treatment felt so random and frustrating to navigate alone. Knowing there might be a specific chemical imbalance helps remove the shame factor significantly :) It validates that the pain is real and measurable not just imagined in someone head. Biofeedback tools seem promising for those who cannot afford expensive hypnosis sessions either. Community support matters just as much as getting the right test results back though ;) Let us keep pushing for better access to these new technologies eventually. Thanks for sharing this insight on the future of diagnostics :)

-
walker texaxsranger April 3, 2026
Big Pharma wants us to believe these biomarkers are the silver bullet while ignoring root causes in food processing and environmental toxins. The vagus nerve theory is convenient for selling antidepressants rather than fixing soil degradation and seed oil exposure. Rome IV criteria were created to expand drug prescriptions under the guise of functional disorder classification. Serotonin reuptake inhibitors do nothing for the actual dysbiosis caused by glyphosate residues in wheat crops. This VisceralSense panel is likely just another revenue stream for corporate medical conglomerates. Real health comes from ancestral diets not synthetic neurotransmitter modulation. Trust your body signals not the algorithmic profiling of corporate medicine.

-
Eva Maes April 5, 2026
Your reductionist view ignores the intricate neurobiology documented in legitimate clinical trials repeatedly. Dismissing validated research as corporate greed shows a lack of engagement with actual pathology mechanisms. The serotonin gradient differences observed in mucosal tissue are quantifiable metrics not theoretical conjecture. Blaming agricultural practices for everything is a classic deflection tactic avoiding pharmacological efficacy data. We need to address the neurological wiring errors causing visceral hypersensitivity regardless of external triggers. Conspiratorial narratives delay necessary treatment for individuals experiencing genuine distress daily. Your skepticism lacks empirical weight when compared to randomized controlled trial outcomes published recently.

-
Debra Brigman April 7, 2026
The gut serves as a secondary heart pumping not blood but feelings through the nervous network. To separate mind from stomach is a false dichotomy imposed by ancient cartesian frameworks failing to grasp modern unity. Our souls digest emotions just as surely as our intestines break down complex carbohydrates chemically. Pain becomes a messenger whispering truths we ignore buried deep within our subconscious layers. Healing requires harmonizing the chaotic symphony of neural impulses firing in silent electric storms below the ribcage. We must listen to the biological poetry written in every spasm and every quiet hour of rest. Existence itself is a fermentation process transforming raw inputs into meaningful experiences constantly.
